

"The worst place to have an epidemic, like a fire, is in close quarters far from help, such as a ship on the high seas. . . . During an epidemic, democracy can be a very dangerous form of Government; the need is for a strong Central authority with a grasp of basic Epidemiology." -Alfred W. Crosby, Epidemic and Peace, 1918
As health exports continue to sound the alarm about the lethal pandemic potential of many natural diseases, including Avian Influenza, Severe Acute Respiratory Syndrome (SARS), and other extremely virulent pathogens released for bioterrorism, naval commanders must prepare to combat lethal epidemics of infectious disease. Unfortunately, effective vaccines and medicines against many of these diseases do not exist, are in short supply, or will not be available in time to prevent widespread death. Virulent epidemics are a strategic and tactical threat, and commanders at every level must be dissuaded from believing that effective countermeasures are simply "medical issues with medical solutions." This sentiment is a faulty appreciation of our vulnerabilities regarding biological threats and invites disaster.
The magnitude of the lineal can he appreciated from an understanding of the Spanish Ru pandemic of 1918 that killed tens of millions of people, primarily in the military age range of 25 to 45 years old. The Navy, Marine Corps, and Army had overlapping regional outbreaks that exploded and receded over a three-month period.1 An estimated 40% of Navy and 36% of Army personnel were sickened, and 50,000 active duty service members died. Training camps ceased to function, ship crews were decimated, and admirals, generals, senior executives, and politicians were incapacitated. Other natural and genetically engineered pathogens are more lethal, can be spread much faster with modern transportation, and their impact on modern society and naval forces can be far greater.
When confronting such biological threats, a commander must decisively implement quarantine and isolation early in an outbreak of virulent disease to maintain the unit's health, prevent the spread of disease, and maintain operational capabilities. Paradoxically, quarantine allows the commander the greatest operational flexibility as the unit is not overwhelmed by illness and death.
The elements of quarantine and isolation are restricting, sequestrating, and cohorting healthy and ill personnel in lime and space to protect susceptible populations. These measures impose severe restrictions on individual freedoms that in "normal" times, are unacceptable in our liberal democracy. Furthermore, faith in modern medicine and our population's relative lack of experience with lethal epidemics can prevent an adequate public-health response to novel biological threats. Even in times of epidemic crisis, civilian leadership is often reluctant to restrict individual rights.
In contrast, commanders routinely issue obligatory and restrictive orders to subordinates to protect their health. This inherent power does not guarantee protection against infectious disease it the orders and/or their execution are fundamentally flawed. In 1918, most commanders instituted "modified quarantine" procedures that the then-surgeon general later described as completely ineffective. A few commanders, through keen foresight, leadership, and judgment, did enact rigorous quarantine procedures that prevented any cases of Spanish Flu in their commands. Case studies of past commanders who won or lost the fight against Spanish Flu are an appropriate introduction to this neglected operational doctrine.
Success in Samoa
In the fall of 1918, Commander John M. Poyer was the military governor of American Samoa. By way of shortwave radio, he learned of the devastating implications of Spanish Flu and its unavoidable arrival in the South Pacific. Without the knowledge or approval of distant superior officers. Commander Poyer instituted a quarantine program for all incoming ships. All debarking personnel were considered infected and immediately segregated from the general population. Potentially sick passengers were isolated in the hospital, and healthy persons were placed under "house arrest" until proven healthy.2
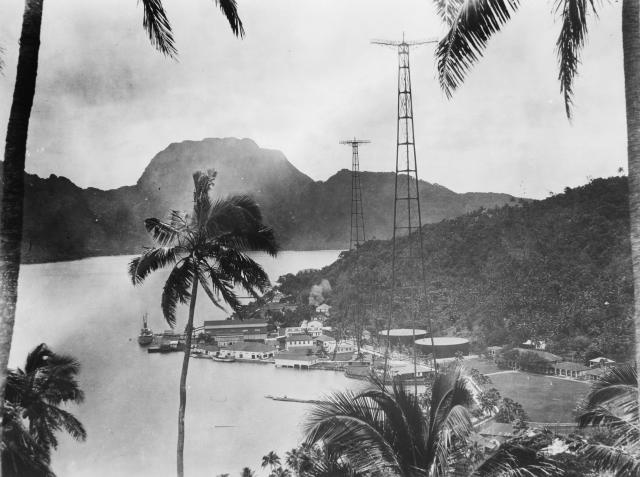
U.S. Naval Institute Photo Archive
Forty miles away, Lieutenant Colonel Robert Logan, the New Zealand Military Governor of Western Samoa, was not as diligent. On 7 November, the steamer Talune was allowed to discharge influenza patients without any restrictions. An immediate epidemic swept his islands, killing 22% of the population of 38,302 within two months.3 On learning of Logan's plight, "Governor Poyer and the United States Navy went to extraordinary lengths to insure against importation of influenza, eventually devising a system of defenses and baffles that only those under direct threat of a deadly epidemic (or under the command of the military) would have tolerated."4 The Samoans, well acquainted with the horrors of imported epidemics, fully cooperated and sustained the quarantine until after the danger had passed.
These measures angered Lieutenant Colonel Logan because Commander Poyer's quarantine interfered with commerce and other functions between the islands. In retaliation, Logan severed the radio link with American Samoa, effectively isolating the island from all outside contact. After the crisis, however, Commander Foyer's efforts were more fully appreciated. He received the Navy Cross and was honored with a 17-gun salute on his relief. In addition, the new governor delivered this commendation in his inaugural address: "He saved your lives and the lives of your brothers and your wives, and thanks to his wisdom you are not bowed down in anguish over the deaths of your children."5 The London Missionary Society expressed "deep appreciation and gratitude to Governor Poyer and the entire Medical Staff of Americans for the prompt and energetic methods adopted by them to prevent the spread of Spanish Influenza in that part of Samoa."6
Disaster in Rio
Half a world away, the cruiser USS Pittsburgh (ACR-4) was limping home from Rio de Janeiro with a complement of dead, sick, and convalescing sailors. The ship's log book records the first death on 13 October: Seaman E. L. Williams died at 1430 from broncho pneumonia with the ship aptly reported as "riding to flood."7 The vessel's commander. Captain George "Blackjack" Bradshaw, had been forced to abandon his mission to interdict German commerce raiders. Had a German warship materialized, the result of the ship action may be surmised by a letter from Admiral William B. Caperton to the fleet surgeon: "On board ship the sick list reached a total of 663 (80% crew attack rate), with a final death toll of 58.8 The efforts of all hands were devoted solely to the care of the sick, and practically the whole ship was given over to them."9
The epidemic on board the Pittsburgh was not the result of bad luck. The progression of Spanish Flu through South America was reported with its specific arrival in Rio de Janeiro on board the steamer Demerara on 17 September. The Pittsburgh's log reveals that working parties went ashore and crew liberty continued as the epidemic in Rio expanded. On 7 October, two flu cases occurred on board the Pittsburgh, and response measures were hastily initiated, though too little, too late, and to no effect.
Commander Poyer and Captain Bradshaw were both commanders of isolated commands who had information that a virulent epidemic was approaching but experienced opposing outcomes. A potential cause for Captain Bradshaw's failure to react effectively can be surmised from historical records. In 1914, Captain Bradshaw had been temporarily suspended for writing an "intemperate" letter to a superior officer.10 Before the epidemic, his crew referred to the ship as the "USS Madhouse." and their service akin to "an inmate aboard Blackjack Bradshaw's floating squirrel cage."11 In previous fitness reports. Admiral Caperton had characterized him as a "very able seaman" although excessively "irritable" and "would prefer to have him serve elsewhere."12 In an adverse fitness report including the Spanish Flu period, the admiral wrote "since October, 1918, I [have noted] instances and acts of great irritation on the part of this officer, particularly in his dealings with subordinate officers."13 It seems clear that Captain Bradshaw was an able seaman, but he was a rigid and difficult officer who simply lacked the ability to react to this novel situation.
On the Dock of the Bay
While Spanish Flu ravaged most shore commands, a few escaped:
The captain of the United States Naval Station on Goat Island, in San Francisco Bay. resolved that he too could keep the disease out. All officers and men attached to the stations were summoned back from the mainland. Guards were placed at the docks with orders to shoot to kill anyone embarking or disembarking without authorization. Crewmen of terries, tugs and supply launches were kept, at gun point, on the far decks of their craft.
An absolute quarantine was imposed upon the encampment of four thousand souls...New trainees or "boots" were ordered to march and. in fact, exist constantly twenty feet from one another...For a week before their training commenced they were sealed off from others.14
By implementing quarantine before unit personnel were infected, the commander retained the initiative to fight the virus at a time and place of his choosing. After eight weeks, the epidemic in San Francisco had subsided, and the base quarantine was lifted. A mere 25 clear cases then occurred and there were no deaths.15 One important factor was that the cases occurred when medical facilities were not inundated by sheer masses of sick, and intensive nursing care could be delivered to each casualty.
When Modern Medicine Is Lacking: Quarantine
The development of effective vaccines has largely halted the virulent epidemics that once swept our nation. However, we cannot afford complacency. Outbreaks of SARS in 2002, ongoing cases of Avian Flu in Southeast Asia, and the prospect of a terrorist attack with natural or manmade pathogens for which no vaccines exist is a growing threat. Fortunately, extensive disease surveillance networks are in place hut are only effective if this information is rapidly disseminated to line commanders and effective quarantine measures are implemented.
In some cases, quarantine polices may only slow the progression of an epidemic. However, slowing the epidemic can have substantial benefits. For example, locally scarce but effective medicines and vaccines can eventually arrive from government stockpiles. Therefore, commanders must fight a battle of time—time to assemble and quarantine the crew before infected: time to slow the spread of the epidemic; time for prophylactic medicines to arrive from distant storage locations; and time for the senior military and civilian leadership to implement an integrated control plan. The time for successful quarantine is short, and local commanders must act decisively before perfect information is available.

U.S. Naval Institute Photo Archive
The focus of a military quarantine is not its application to sick individuals, but to healthy military units. If rapidly implemented at the unit level, quarantine can limit the spread and impact of a virulent disease and preserve the fighting strength of the naval services. Speed and execution are essential. While commanders can easily lift quarantine, pathogens cannot he dislodged by decree. Four synergistic concepts create an effective quarantine: restriction of movement, sequestration of the healthy, cohorting of personnel, and isolation of sick.
Restriction of Movement. As a virulent outbreak is evolving into an epidemic, service members should be immediately recalled to their ship or duty station. Further interactions must be tightly choreographed to prevent transmission of the disease. Movement restrictions must apply to bases, units, and individuals, and personnel transfers must be rescinded. Units should receive only critical supplies by drop-delivery at designated locations for pick-up, or by transfer using underway replenishment techniques. Command and control functions, such as commander's call and staff meetings between commands, should be by phone, conference calls, emails or radio.
Sequestration. Once an adequate period of lime has elapsed for personnel to reach their designated location, sequestration must begin. Physical separation of units is generally the most effective method with the smallest risk for breaches in transmission security. For example, ships can sortie, and shore units can occupy a particular building or camp, or be assigned specific training ranges for field billeting. To protect healthy units, particularly operational forces, commanders should task individuals from infected units to care for the sick.
Cohorting. Initially, the smallest unit capable of relative self-sufficiency such as ships, squadrons, and companies should be considered a cohort. Early in an outbreak, each cohort must be sequestered. As these cohorts are deemed disease-free (no infections within the incubation period), larger parent commands can be created.
Isolate the Sick. Sick patients, exposed individuals, and affected units should be isolated into cohorts, sequestered, and their movements restricted. Transporting highly infectious patients through the existing Department of Defense (DoD)/Navy medical evacuation system will likely infect additional units in a domino effect. In a true epidemic, an evacuated patient may not reach their intended destination nor benefit if delivered to a medical treatment facility overrun with other victims. Given the highly infectious nature of these diseases, the affected unit will not avoid an outbreak by jettisoning its early cases. A more sensible strategy is to retain index cases in the affected unit, implement internal control procedures, and drop-deliver medical supplies and personnel if available.
Quarantine First, Modify Later

U.S. Navy
The U.S. Navy's efforts to control the Spanish Flu epidemic were largely abysmal-as were the efforts of the Army, Public Health Services, and civilian authorities. Palliative control measures proved worthless, such as recommendations to restrict travel "to a minimum consistent with the requirements of war." enacting "modified quarantine" policies, keeping your "vitality close to par," and sleeping with your windows open. (See Figure 1) These half measures failed miserably and merely added inconvenience to the grim proceedings of burying the dead and crowding the sick into overflowing hospitals and sick bays. Despite the benefits of modern medicine, communication, and logistical infrastructure, the commander must resort to quarantine and isolation when lethal infectious diseases emerge.
Currently, epidemic response plans are in an early stage of development. Of these. DoD Directive 5200.8, "Security of DoD Installations and Resources." and DoD Directive 6200.3 "Emergency Health Powers on Military Installations," must be understood by every commander. The provisions contained in these directives are powerful tools that reiterate the authority, responsibility, and accountability of commanding officers. Strong and forceful execution by the commander is an absolute requirement.
When a virulent epidemic emerges, commanders must restrict, sequester, and cohort personnel in time and space. The main effort must be to protect and support combatant commanders and units that are disease free. Assuming a strong defensive posture in the face of a lethal epidemic deprives the disease of the initiative. Captains must recall the away parties, pull up the gangplank, and prepare to repel borders. A new war is upon us, and how we respond will determine if we are able to serve our Sailors, loved ones, ships, and country.
1 Annual Report of the Navy Surgeon General, 1919, p. 355, 374-375.
2 Alfred W. Crosby, Epidemic And Peace, 1918 (Westport: CT: Greenwood Press, 1976), p. 121, 236-239.
3 Ibid. pp. 236-239.
4 Ibid. p. 238.
5 Crosby, p. 239 reference 31, National Archives, San Francisco, R.G. 284, Subject Files 1900-42, Medical Reports, Alex Hough to Commander Poyer, Apia, 14 February 1919.
6 Ibid, p. 2.19 reference 32, Pago Pago O Le fa' atonu, vol. 17 (July 1919).
7 National Archives, Washington DC., Ship Log Section, Log of USS Pittsburgh, 13 October 1918.
8 National Archives, Washington D.C., R.G. 52, Records of the Bureau of Medicine and Surgery, Box 511, 127278-127285, letter E. R. Stitt, SG USN, dated 17 December 1920.
9 National Archives, Washington D.C., R.G. 52, Headquarters Records Correspondence 1842-1941, Box 555, 192222, letter Commendation Fleet ADM W. B. Caperton, dated 10 April 1919.
10 National Archives, Washington D.C., Officers Fitness Report Section, Naval Examining Board Re. Bradshaw, George B., dated 13 October 1916.
11 A. A. Hoehling, The Great Epidemic (Boston: Little, Brown and Company, 1961) p. 127.
12 National Archives, Washington D.C., Officers Fitness Report Section, Report of the Fitness of Officer, Bradshaw, George B., period(s) 1916-1919.
13 National Archives, Washington D.C., Officers Fitness Report Section, Report of the Fitness of Officer, Bradshaw, George B., period 1 Oct 1918-30 April 1919.
14 Hoehling, p. 35.
15 Annual Report of the Navy Surgeon General, 1919, p. 428.